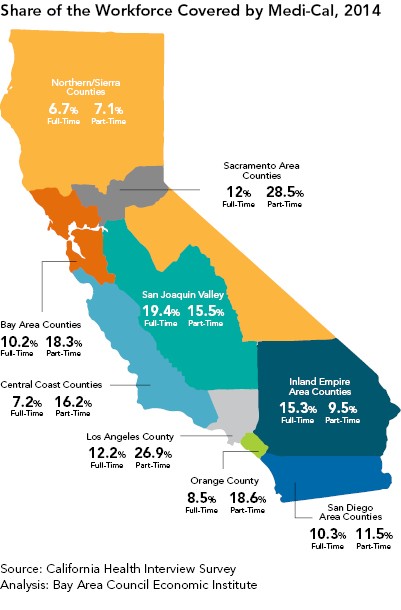
California is a large state made up of several distinct regions. Following the Great Recession, the economic recovery in the state has been uneven. Coastal regions such as the Bay Area, San Diego, and Orange County have seen impressive growth, while inland regions such as the San Joaquin Valley and North State have lagged behind. Average earnings in these regions are also very different; hence higher shares of employed individuals are eligible for Medi-Cal in some regions than in others. Rates of Medi-Cal enrollment among the employed therefore vary significantly across the state.
The North State, Central Coast, Orange County, San Diego and Bay Area regions have the lowest shares of full-time employed individuals enrolled in Medi-Cal. With the exception of the North State, these regions have done very well coming out of the Great Recession, recording low unemployment and a high number of well-paying jobs. By contrast, the San Joaquin Valley, the Inland Empire Area, Los Angeles County, and the Sacramento Area have higher rates of Medi-Cal enrollment among the employed. This is due to their higher proportions of lower- to middle-income jobs that do not provide health benefits. In the North State, the low share of working Californians covered by Medi-Cal is somewhat surprising. These rates are a result of relatively higher percentages of unemployment and high rates of uninsurance, though, rather than robust growth and higher wages. Of the relatively smaller percentages in this region who are employed and covered, fewer are enrolled in Medi-Cal.